U.S. Response to the 2001 Anthrax Incidents — Erin C. Hoffman
INTRODUCTION:
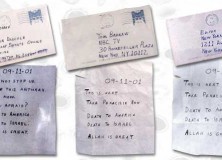
The anthrax attacks during September and October 2001 caused widespread panic across the United States. Still recovering from the attacks of 9/11, the fragile American public became increasingly fearful of the threat of terrorism in the United States. As public anxiety grew, so did the number of suspicious reports, which only hampered response efforts. Conflicting reports from within the government regarding the Anthrax attacks provoked this sense of fear. With over 20 federal agencies having a role in responding to the public health and the medical consequences of a bioterrorist attack, there was a great deal of confusion and uncertainty surrounding the necessary response. Thus, the U.S. government faced the daunting task of not only managing an increasingly fearful public, but also developing and implementing new protocols in an effort to respond to these unprecedented attacks. A majority of analysts characterize the anthrax response effort as both a failure and a valuable learning experience.
STRATEGY:
Although some pre-existing relationships between federal, state, and local public health plans contributed to a state of semi-readiness, the response to the 2001 anthrax attacks required venturing into unfamiliar territory for many public health and law enforcement officials. Because of this, planning was done mid-response and typically executed in an ad hoc manner, including the formation of two new organizations, the Mail Security Task Force and the Unified Incident Command Center, to assist in managing the response to the anthrax attacks.
INTEGRATED ELEMENTS OF NATIONAL POWER:
Bureaucratic tensions (mostly between the public health agencies and the criminal investigative authorities) created some instances of shortcomings in strategy development and implementation. For example, while public health agencies tend to have an inductive approach to investigations, law enforcement follows a deductive approach. This caused frustration on both sides, especially pertaining to evidentiary issues and a lack of information sharing. While bureaucratic conflict often obstructed components of the response effort, the implementation of new ad hoc organizations such as the Unified Incident Command Center (UICC) showed the willingness of many U.S. government actors to pool their resources to create a more fluid response.
EVALUATION:
The variables that most significantly affected the response efforts in a negative manner were a lack of a clear authority; the presence of conflicting and inconsistent information; a lack of personnel, equipment, and funds; and surrounding legal issues, such as the lack of contractual authority. Other variables that weakened the U.S. government response included the inability to use certain resources due to the lack of a declared national emergency, and the challenge of adressing conflicting views from the public health community and the criminal investigation authorities. While there were many weaknesses in the response, there were some strengths as well. These include agency ingenuity and flexibility in creating new ad-hoc organizations with sufficient authorities to have a significant impact, and ad hoc UICC cooperation where agencies proved willing to use their expertise to advise others in impromptu policies.
RESULTS:
While the literature does not emphasize the economic cost of insufficient interagency coordination during the response, it is clear that such costs arose due to a lack of communication between agencies. For example, additional costs were caused by duplication of efforts and an unnecessary directed focus from organizations who should not have had a role in the response activities. Indirect expenses also included the filling of unncesseary antibiotic prescriptions for the uninformed public. Insufficient coordination also led to the inability to calm fear, and additional coordination may have prevented unnecessary loss of lives. However, while insufficient coordination caused a multitude of problems in the months and years after the anthrax attacks, it also led to significant reform-oriented legislation such as The Public Health Security and Bioterrorism Response Act of 2002, and to the establishment of new strategic plans for a variety of involved organizations.
CONCLUSION:
The necessity of planning and coordination, the importance of effective communication (both among responders and the general public), and the critical importance of a strong public health infrastructure to serve as the foundation for bioterrorism response efforts can all be seen in this case study. Overall, the U.S. government was not prepared for the extent, pace, and complexities of the the 2001 anthrax attacks. This lack of preparation caused unnecessary confusion and panic in an already difficult situation. However, often neglected federal, state, and local health agencies routinely worked at the limits of their capacity with admirable results. These public health professionals and individual clinicians were able to provide much needed services throughout the anthrax scare.